Protection Risks During COVID-19: Negotiating Safe Access to Gender-Based Violence Services in The Rohingya Refugee Response in Cox’s Bazar
The COVID-19 crisis has significant protection, health and socio-economic implications for the Rohingya refugee response. Nearly one million Rohingya refugees live alongside some of the most at-risk host communities in southern Bangladesh, a disaster-prone region already vulnerable to a wide-range of shocks and stresses, as well as domestic and gender-based violence.
Gendered Effects and Protection Risks in Bangladesh During the COVID-19 Lockdown
Since the lockdown was imposed and critical humanitarian activities re-defined in late March, humanitarian actors are struggling to negotiate access to communities at the advent of monsoon and cyclone season, making for an increasingly complex and multi-layered protection environment with intersecting risks related to COVID-19. There are also a number of gendered effects related to COVID-19 that disproportionately affect at-risk women and girls across refugee and host communities as well as their safe access to life-saving gender-based violence services.
National lockdown, restriction of movement, quarantine, isolation and community shielding measures are likely to negatively impact household tensions as the crisis becomes increasingly protracted, further restricting the movement of women and girls and their access to already limited services while contributing to an increase in intimate partner and domestic violence risks and violence against children. The COVID-19 response has overstretched the capacity of the health sector which raises key concerns related to the interruption of critical and life-saving sexual and reproductive health and gender-based violence (GBV) services. Further mobility restrictions for women and girls have affected their access to service points, making safe case follow up an increasingly challenging activity. Moreover, the recent government restrictions have narrowed the scale and range of humanitarian operations permitted during COVID-19, which has impacted access to communities and the available referral pathways of support. As service providers reduce their field presence, the humanitarian space is shrinking, which is one of the biggest protective factors for affected communities.
Negotiating Safe Access to GBV Services and Adaptation of Modalities
GBV remains a major concern in Cox’s Bazar and negotiating GBV-related programming whether prevention, risk mitigation or response, is an on-going process that requires a multi-pronged approach working with local government authorities and communities. Three years into the humanitarian response, GBV specialists are more familiar with field-level negotiations which have had significantly more ‘buy-in’ at the community level, multi-sectoral services, referral pathways, community groups and engagement strategies. Negotiating GBV programming with local authorities at the camp level has always been challenging and constantly evolving. Within the current restrictions, GBV specialists have managed to negotiate some program components as ‘critical’ during COVID-19 which are more response-oriented and have adapted programming where possible.
Some protection actors have adapted their activities with remote approaches such as hotline or phone counseling. Yet, for GBV specialists such modalities can create new risks and are limited in scope since many women and girls do not have safe access to a phone. Key to note that relying on hotlines is precarious, given that Rohingya refugees are not legally allowed to access local SIM cards and telecommunications blackouts are frequent across the camps. Given such challenges, GBV actors have managed to negotiate the inclusion of certain ‘life-saving’ activities, specifically ensuring that in-person case management services are able to continue, usually embedded at service points in women and girls safe spaces or within health facilities. Although this is a significant achievement for the GBV sector given the restrictive operational environment at present, challenges continue to persist. For example, the fifty percent reduction in staffing due to ongoing government lockdown restrictions affects the quality of care and with this new status quo of ‘one caseworker per facility’ supervisors are concerned around quality of care, burnout of caseworkers and lack of adherence to interagency GBV minimum standards in emergencies. Community-level GBV prevention and outreach activities have been side-lined, to focus on COVID-19 awareness-raising.
Psychosocial support and life skills activities for women and girls have also managed to continue so long as they focus thematically on COVID-19. GBV specialists have had to become more innovative in their approaches given that it is essential to maintain non-case management services in such centres to ensure it remains a safe, non-stigmatizing space for women and girls and does not risk becoming a “GBV centre.” For example, tailoring and sewing classes, though interrupted at the onset of COVID-19, have been able to resume while adhering to physical distancing guidelines. Trained women and adolescent girls were able to maintain their skill development, now sewing masks for their communities and families.

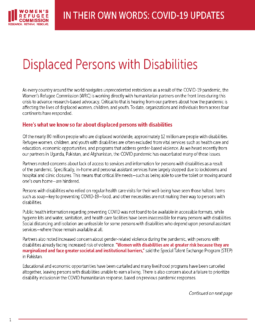
IOM Protection conducts GBV risk mapping during monsoon season in Camp 9, Cox’s Bazar, Bangladesh (Photo credit: Rawshan Zannat/IOM)
Despite some recent inroads, rumors, fears and misinformation related to COVID-19 continue to impact access to services and there are increasing restrictions observed in the movement of women and girls in public space that hinder safe case follow up. GBV specialists have to consistently reiterate that lower reporting should not be misconstrued as a reduction in GBV. On the contrary, the absence of prevalence data coupled with observations from case management service providers is disconcerting for GBV specialists on the ground and much effort has been made between interagency technical working groups to strategically adapt interventions, closely monitor intimate partner violence cases and roll out GBV prevention curriculum framed as a ‘critical’ risk mitigation activity as part of COVID-19.
Disaster Preparedness: An Emerging Best Practice
Building upon past experiences and learning between GBV risk mitigation and disaster risk reduction, some key strategies have been adapted to respond to the dual challenge COVID-19 brings during monsoon season. The women’s committee in Teknaf, consisting of Rohingya and Bangladeshi women served as a best practice model. Trained as first responders, last year they played a key role in ensuring the most at-risk households and individuals were included in early warning and response mechanisms and developed household evacuation plans requiring specialized assistance to persons with mobility issues as well as safe referral of protection and GBV cases. IOM’s GBV outreach teams are framing COVID-19 as a similar risk akin to the more familiar shocks and stresses such as flooding, landslides and cyclones to develop household preparedness plans and is planning to repurpose existing community-led structures and skilled community groups towards supporting such efforts. Working alongside communities is crucial given the numerous concerns for individuals and communities (i.e. what to expect if someone is quarantined, being separated by loved ones amidst increasing tensions, rumors and fears). Integrating COVID-19 as ‘another risk to plan for’ can be a more holistic, practical approach to engage individuals and communities and maintain strong protection and GBV lens to risk mapping and action planning.
GBV specialists are also preparing for further access restrictions by strategically aligning with health teams. For example, the model of mobile medical response teams, activated usually in the immediate onset of a disaster, has embedded GBV focal points and will receive further training in light of COVID-19. GBV focal points will now be working in recently constructed quarantine facilities and isolation and treatment centres (ITCs) that have dedicated counseling rooms for protection.
Challenges to Deliver GBV Services in Line with The COVID-19 Response
It is key that governments, partners, and donors work under the assumption that GBV is occurring in all crises and that reliable prevalence data on the scope of GBV is not needed to design appropriate interventions. GBV data is and will always be difficult to obtain, due to insecurity, service gaps, lack of protection of survivors, fear of reprisals and impunity for perpetrators, social stigma, perceptions and cultural norms around sexual violence and community pressure over survivors. GBV services are life-saving and should be considered an equally critical part of the COVID-19 response. That said, these services should not focus only on ‘response’ or supporting survivors but also on a wide-range of complementary risk mitigation and prevention activities which will need to be adapted in light in COVID-19 prevention measures but cannot stop altogether.
Negotiation at the national level is now more imperative than ever to ensure access and maintain a protective environment for affected communities amidst evolving risks ranging from increased violence, abuse and exploitation, human trafficking, child protection and gender-based violence.
Read the full story here!